

Are Americans feeling better or worse since the 1970s and does this pattern vary by gender and race? Jason L. Cummings explores U.S. trends in self-rated health inequalities over the last five decades (1972-2018).
While survival, or differential survival, is a traditional topic of interest in socio-demographic studies, the issue of life quality, and differential life quality, has gained momentum in recent years. Self-rated health (SRH) refers to an individual’s subjective assessment, experience, or perception of their own health status. An excellent proxy of overall health, morbidity (sickness) and mortality later in life, SRH represents a valuable tool in public health monitoring and demographic research.
Quantifying well-being: metrics, meaning, and the human experience
In the United States, African Americans generally report poorer health than their White American counterparts, with some reductions in the racial gap from the 1970s to the early 2000s (Cummings & Jackson, 2008; Hughes & Thomas, 1998; Yang & Lee, 2009). On the other hand, studies on the gender gap in health status reveal that women have made significant strides in well-being since the 1970s, with SRH disparities narrowing and reaching parity by the early 2000s (Cummings & Jackson, 2008; Schnittker, 2007). While these studies have advanced our knowledge regarding U.S. patterns and trends in SRH over time, they are in part limited, because they:
1) only examine SRH trends prior to the 2007-2009 U.S. Great recession, or
2) pay little attention to how racial disparities in health vary by gender (Bowleg 2012)
These limitations are important because in the years since the recession, well-being patterns in the United States have worsened, with general declines across a range of social indicators of quality of life (e.g., happiness, levels of worry, stress, and pain; Cummings 2020; Deaton 2012) coupled with well-publicized increases in so called “Deaths of Despair” or preventable health conditions linked to despair and hopelessness, such as suicide, and opioid-alcohol related-mortality, affecting the U.S. White population in particular (Case and Deaton 2020).
The racial and gender dynamics of how Americans assess their own health
In a recent paper (Cummings 2023), leveraging data from the General Social Survey (GSS) between 1972 to 2018, I examined trends in SRH at the intersection of race and gender. Two key questions guided my study:
1) What is the pattern of racial and gender disparities in SRH from 1972–2018?
2) Did racial and gender disparities in SRH from 1972–2018 decrease, increase, or remain unchanged?
Results show that while African American women and men express feeling healthier today than they did in the 1970s, and White women report feeling about as healthy as back then, White men report feeling comparatively worse. The pattern of decline in SRH experienced by White men was most pronounced after the recession (continuing through the economic recovery).
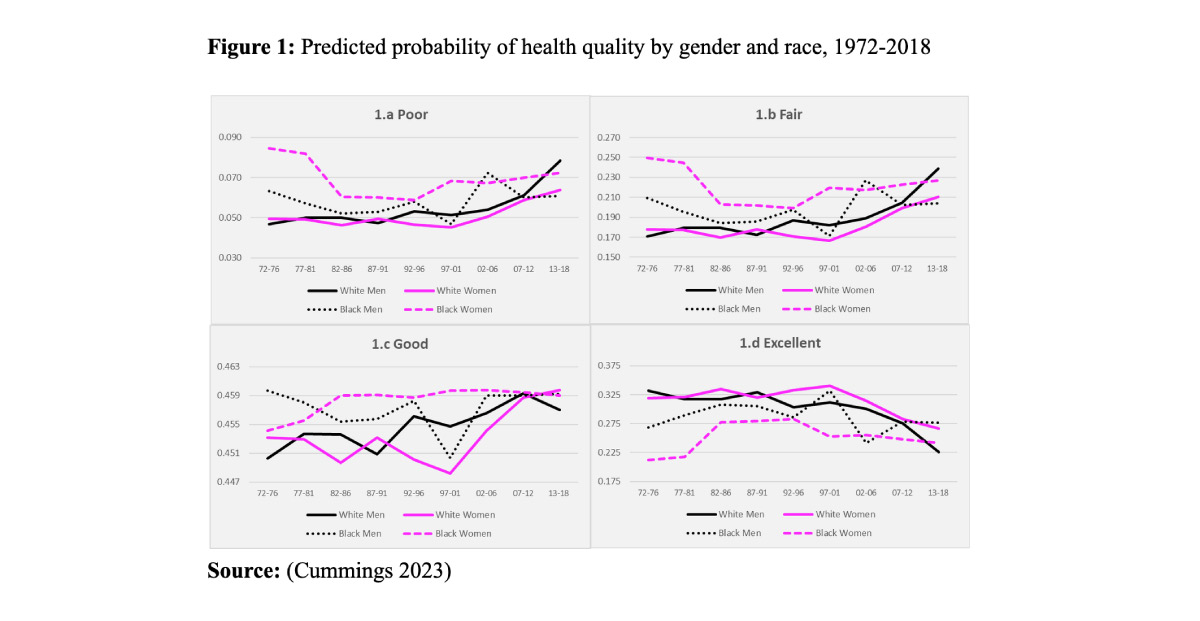
Figure 1 reports predicted probabilities across each outcome category (i.e., poor, fair, good, excellent) based on regression models adjusting for group differences across a range of sociodemographic factors (e.g., age, region, marital status, employment, education, household income, and occupational prestige). The lines illustrate a trend of virtual convergence in SRH disparities from the early 1970s to the late 2010s across demographic groups, with only one exception—“good health”—which remained largely unchanged over time and across groups. The most notable change in health status over time occurs at the upper bound of SRH (“excellent health”, panel d). For example, the likelihood of reporting “excellent health” declined significantly for White men and women from the early 2000s (–30% and –16%, respectively). In contrast, African American men and women showed a general pattern of improvement, with increases of 4% and 14%, respectively, in the likelihood of reporting “excellent” SRH.
Socioeconomic attainment (e.g., having a high income or education) and work (e.g., being employed or having a job with high occupational prestige) were primary factors that protected or improved the health status of all groups, but the strength of the positive impact of these factors on good or excellent health differed depending on gender and race (Cummings 2023). For example, the benefit of being a high-income earner, having a college degree or being employed full-time appeared to be more protective to the health status of White women and men, while for African American women and men, having a job with a high occupational prestige was more protective.
Conclusions
The findings of this paper coincide with an interdisciplinary body of research demonstrating declines in the quality of life of White Americans since the recession. This finding appears to exist across objective indicators of well-being like mortality and life expectancy (Case & Deaton, 2015). Similarly, I find that SRH disparities have followed a pattern of convergence, with African American women and men witnessing gains in their SRH status since the 1970s. In contrast, White women overall have experienced little to no change in their health status and White men have experienced absolute declines. Perhaps even more surprisingly, however, the unparalleled pattern of decline in SRH experienced by White men was most pronounced after the recession (continuing through the economic recovery). This finding may suggest that the health status of White men was not simply shaped by economic forces brought on by the recession in real time, but possibly by other forces most likely preceding the 2016 U.S. presidential election, i.e., the election of the first African American U.S. President. This explanation aligns with the work of Malat, Timberlake, and Williams (2011), demonstrating immediate improvement in self-rated health among Blacks preceding the election of President Obama, but no such change or improvement in the health status of Whites.
This work also coincides with my own previous work (see Cummings, 2020) which also found an unprecedented pattern of decline in happiness among the White male population after the Great Recession, which parallels their greater relative decline in financial happiness. Although White Americans did not suffer greater financial or job loss during the Great Recession than their African American peers (the opposite is the case), White Americans (but especially White men) may have “perceived” that their financial loss was greater, and perhaps that they were primary victims of the economic downturn, in part leading to declines in their well-being.
References
Beck, A. N., Finch, B. K., Lin, S.-F., Hummer, R. A., & Masters, R. K. (2014). Racial disparities in self-rated health: Trends, explanatory factors, and the changing role of socio-demographics. Social Science & Medicine, 104, 163–177.
Bowleg, L. (2012). The problem with the phrase women and minorities: Intersectionality—An important theoretical framework for public health. American Journal of Public Health, 102(7), 1267–1273.
Case, A., & Deaton, A. (2015). Rising morbidity and mortality in midlife among white non-Hispanic Americans in the 21st century. Proceedings of the National Academy of Sciences, 112(49), 15078–15083
Cummings, J. L. (2020). Assessing U.S. racial and gender differences in happiness, 1972–2016: An intersectional approach. Journal of Happiness Studies, 21(2), 709–732.
Cummings, J. L. (2023). Entangled Inequalities: U.S. Trends in Self-Rated Health at the Intersection of Gender and Race, 1972–2018. Social Indicators Research, 169, 759–774 (2023)
Deaton, A. (2012). The financial crisis and the well-being of Americans 2011 OEP Hicks Lecture. Oxford Economic Papers, 64, 1–26.
Hughes, M., & Thomas, M. E. (1998). The continuing significance of race revisited: A study of race, class, and quality of life in America 1972–1996. American Sociological Review, 63, 785–795.
Malat, J., Timberlake, J., & Williams, D.R. (2011). The Effects of Obama’s Political Success on Self-Rated Health of Blacks, Hispanics, and Whites. Ethnicity & Disease. 21 (3): 349-355.
Schnittker, J. (2007). “Working more and feeling better: women’s health, employment, and family life, 1974-2004.” American Sociological Review 72 (2): 221-238.
Yang, Y., & Lee, L. C. (2009). Sex and race disparities in health: Cohort variations in life course patterns. Social Forces., 87(4), 2093–2124.