

While public health officials worry about the distressingly high levels of tobacco use across the world, they increasingly recognize that smoking also worsens inequalities in health and life expectancy.
Trends in smoking inequalities come from multiple sources and present challenges for anti-tobacco policies. Among the several sources of differentiation, we will consider gender, education, cohort, and age in France and the United States (Pampel et al., 2017).
Patterns of change
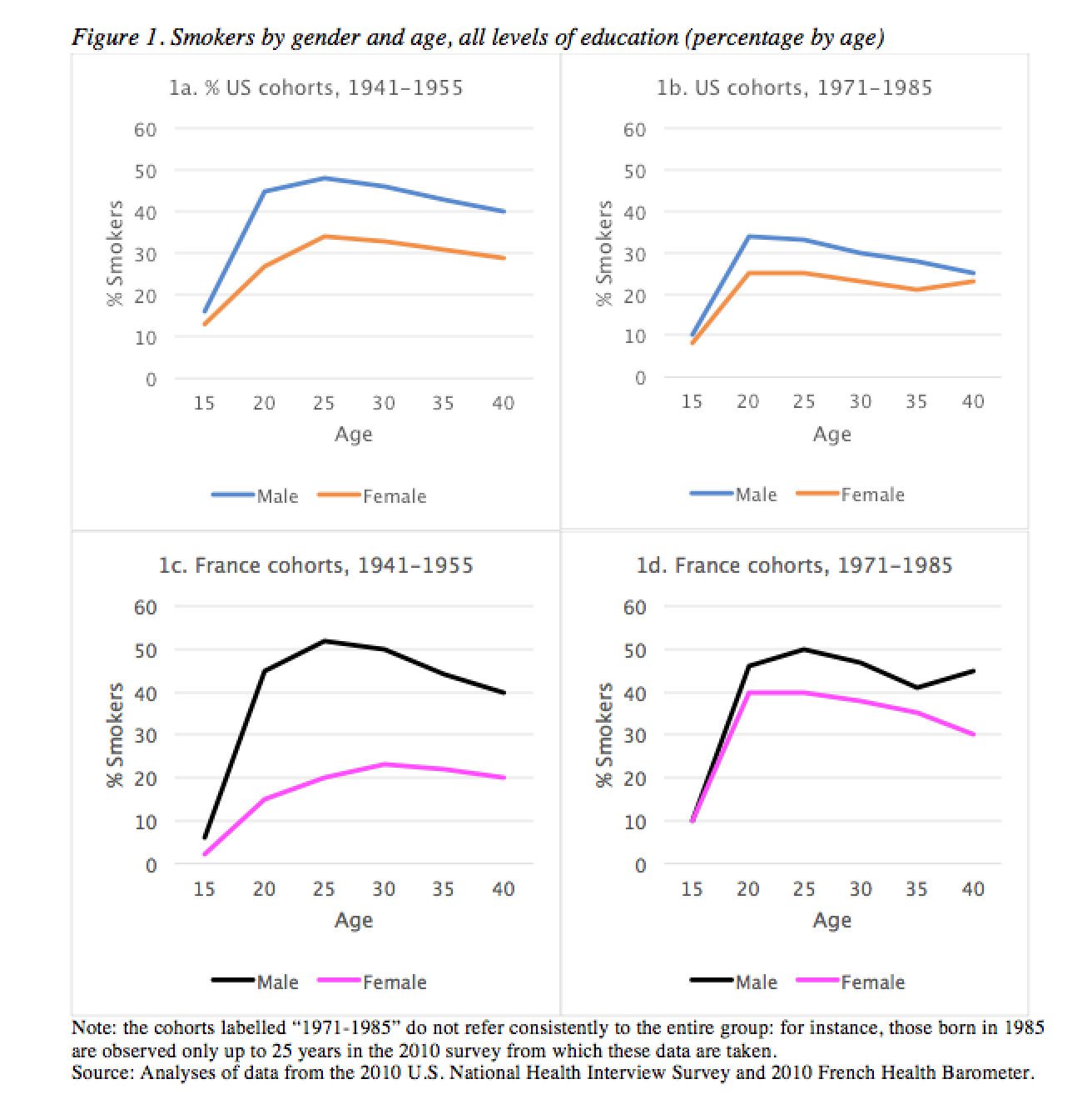
Figure 1 illustrates the nature of differences in smoking by gender, cohort, age, and country. Smoking at each age is based on the recall of the starting and stopping age. The graphs first demonstrate convergence across cohorts in prevalence of male and female smoking. Compare the gender differences across the older cohorts (born 1941-1955) with those for the younger cohorts (1971-1985). In the United States and particularly in France, the large gap between men and women narrows considerably. This reflects the slower decline in smoking among women.
The graphs also illustrate changes over the life course. For the younger cohorts, the gender gap is small in adolescence – rates reach near parity before age 20. By young and middle adulthood, male smoking is considerably higher in both countries.
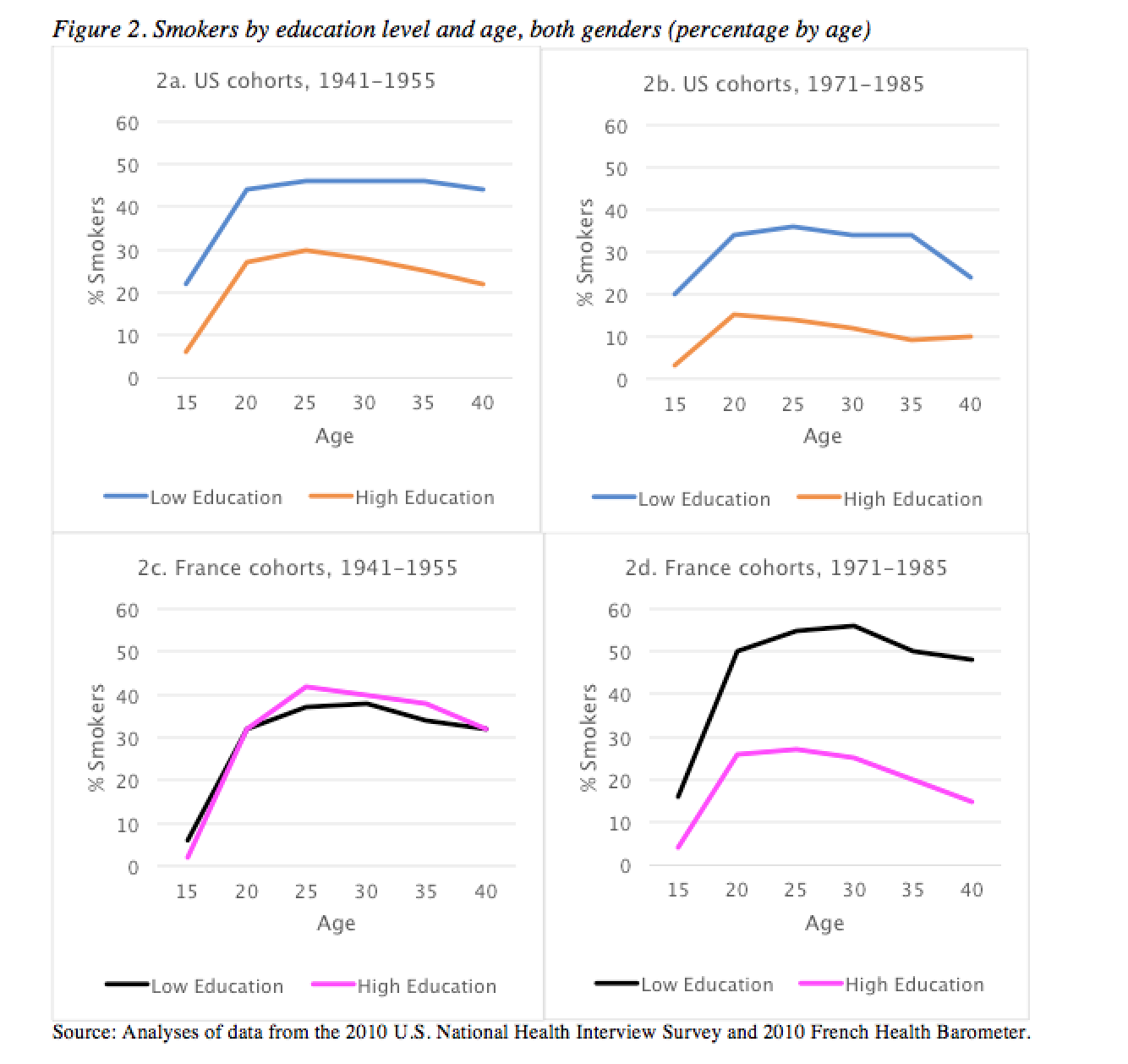
Figure 2 presents the same graphs for low education (less than secondary school) and high education (college degree). Education refers to completed level at the time of the survey, while smoking at each age is again based on the recall of the starting and stopping age. Note that the gap in smoking across the education groups gets larger for younger cohorts in both the United States and France, but the change in France is particularly striking. Note also that the gap increases with age. The educational advantage starts small but gets bigger as the cohorts get older. Together, the rising disparities across cohorts and ages mean that low education groups are most disadvantaged relative to high education groups among adults in younger cohorts.
These trends emerge earlier in the United States than in France. The gender gap narrowed sooner in the United States, as the oldest cohorts in France show much higher smoking among men than women. The educational gap similarly widened sooner in the United States.
Implications for Inequalities in Health
Despite declining use of cigarettes in most Western countries, the toll of tobacco use for mortality remains troublingly high (Thun et al., 2003). Even after anti-tobacco campaigns, clean air regulations, and widespread knowledge of the harm of tobacco, smoking persists. About one-fifth to one-third of adults smoke in the United States and Europe. In the United States between 2005-2009, an estimated 480,000 annual deaths or about 20% of all deaths were tobacco-related (U.S. Department of Health and Human Services, 2014). In France in 2010, an estimated 69,700 deaths or about 19% of male deaths and 6% of female deaths were tobacco-related. In Europe, an estimated 16% of all deaths of adults age 30 and over are due to smoking (World Health Organization, 2016). These figures show that smoking is the single most preventable cause of death in the United States and France (and, indeed, many European countries).
The trends in smoking inequalities that we have shown correspond to changes in mortality. The gap in mortality rates between low and high education groups has been steadily growing in many countries, much as it has for tobacco use. A somewhat different trend has occurred for women and men. The extension of life expectancy among women has slowed relative to men. The slowing has reduced the male disadvantage but, less positively, has limited the gains to women, mirroring the gendered trends in smoking. Given the current patterns and slowly accumulating harm of smoking, the gender- and education-based trends in mortality will persist into the future.
Educational and gender disparities in smoking can emerge in two ways that are familiar to demographers. First, they emerge across birth cohorts or generations. Each new cohort enters an environment in which attitudes and behaviors have changed. In older cohorts, smoking was widely popular among men, but less acceptable for women; educational disparities were small but gender disparities were large. Younger cohorts, in contrast, have entered an environment with lower smoking and stronger anti-smoking attitudes. Highly educated men have reduced smoking the most, while the decline for less educated men and women overall has been smaller.
The second source of changing disparities relates to age. Smoking levels change from adolescence to early and middle adulthood. Many teens start smoking but many also quit as they get older. Adult experiences can in this way redirect adolescent smoking trajectories and reshape gender and education disparities.
The cohort and age patterns also differ across countries. In France, the smoking epidemic began later than in the United States. For example, the number of cigarettes sold per adult per day peaked in the United States in 1961, while it peaked considerably later in France in 1985. As a result, smoking prevalence is higher today in France (31%) than the United States (16%). These country differences affect gender and educational disparities. Other European countries such as Italy show similar changes in the level of smoking (Ipsen, 2016) and likely show similar changes in inequalities in smoking.
These findings on smoking and mortality disparities suggest the value of anti-smoking policies that target specific groups. Broad interventions such as raising tobacco prices and restricting tobacco use in public places have lowered overall smoking prevalence in the United States and France. However, the growth of inequalities in smoking suggests the need for something more (Frolich and Potvin, 2008), for programs tailored to less educated groups that have the highest smoking rates. For gender, men still smoke more than women, but the slower drop in tobacco use among women suggests they may also benefit from targeted programs.
References
Frohlich K.L., & Potvin, L. (2008). The inequality paradox: The population approach and vulnerable populations. American Journal of Public Health, 98, 216–221.
Ipsen C. (2016). Smoking in Italy since World War II. N-IUSSP, May 2, 2016.
Pampel F.C., Bricard, D., Khlat, M., Myriam, & Legleye, S. (2017) Life course changes in smoking by gender and education: A cohort comparison across France and the United States. Population Research and Policy Review, 36(3), 309-330.
Thun, M.J., Carter, B.D., Feskanich, D., Freedman, N.D., Prentice, R., Lopez, A.D., … Gapstur, S.M. (2013). 50-Year trends in smoking-related mortality in the United States. New England Journal of Medicine, 368, 351–364.
Tobacco Atlas Country Fact Sheet: France. (2015).
U.S. Department of Health and Human Services. 2014. The Health Consequences Of Smoking: 50 Years Of Progress: A Report Of The Surgeon General. Atlanta: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health
World Health Organization. (2016). Deaths from tobacco in Europe.